Fill Out a Valid Virginia Police Crash Report Template
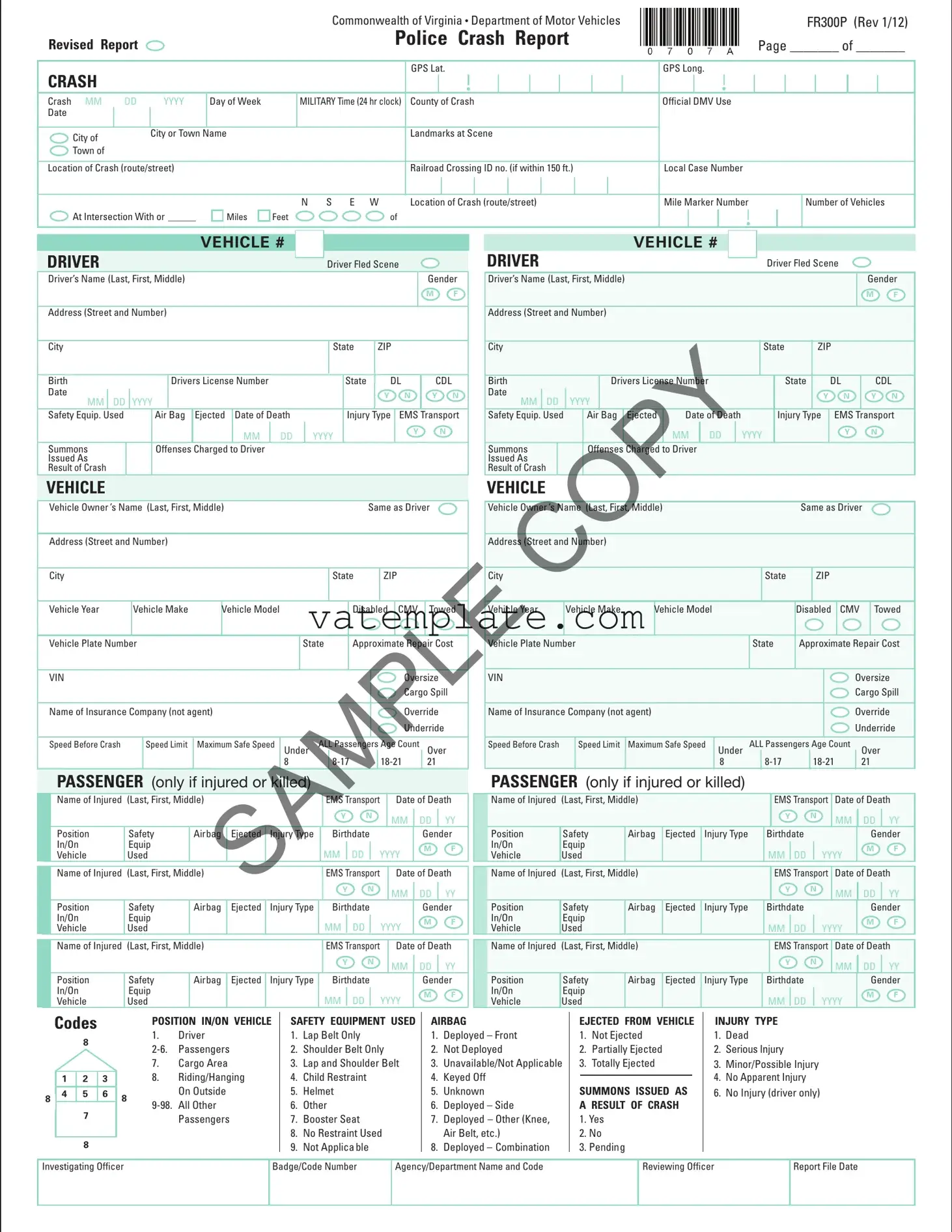
The Virginia Police Crash Report form, formally recognized by the Commonwealth of Virginia Department of Motor Vehicles as FR300P, serves as a comprehensive document for recording details of vehicular incidents within the state. Revised in January 2012, this form meticulously captures a wide array of data, ranging from basic information – such as the date, time, and location of the crash – to more detailed descriptions encompassing vehicular specifics, driver and passenger details, conditions leading to the crash, and resultant damages or injuries. It also includes sections tailored specifically for commercial vehicle incidents, highlighting elements like vehicle configuration, cargo type, and hazardous material information if applicable. Designed to assist law enforcement officers in documenting the multifaceted nature of road incidents, the report serves multiple purposes: it helps in the investigation process, aids in the statistical analysis of road safety measures, and supports the adjudication of any legal matters arising from the crash. Moreover, the form incorporates a diagram section for visual representation of the crash scene, alongside a narrative space for a detailed crash description, ensuring a thorough record is maintained for future reference. This meticulous approach to crash reporting underscores Virginia's commitment to road safety, legal clarity, and the provision of accurate data for improving future road use policies.
Virginia Police Crash Report Example
|
|
|
|
|
|
|
|
Commonwealth of Virginia • Department of Motor Vehicles |
|
|
|
|
|
|
|
|
|
FR300P (Rev 1/12) |
||||||||||||||||
Revised Report |
|
|
|
|
|
|
Police Crash Report |
|
|
|
|
|
|
Page _______ of _______ |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CRASH |
|
|
|
|
|
|
|
|
GPS Lat. |
GPS Long. |
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Crash MM |
DD |
YYYY |
Day of Week |
|
MILITARY Time (24 hr clock) |
County of Crash |
Official DMV Use |
|
|
|
|
|
|
|
|
|||||||||||||||||||
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City of |
|
City or Town |
Name |
|
|
Landmarks at Scene |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Town of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Location of Crash (route/street) |
|
|
|
|
|
|
Railroad Crossing ID no. (if within 150 ft.) |
Local Case Number |
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N S E W |
Location of Crash (route/street) |
Mile Marker Number |
|
|
|
|
Number of Vehicles |
|||||||||||||||||||
At Intersection With or ______ |
|
|
Miles |
|
Feet |
of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
DRIVER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Driver Fled Scene |
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Driver’s Name (Last, First, Middle) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Address (Street and Number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
ZIP |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Birth |
|
|
|
|
|
Drivers License Number |
|
|
|
|
|
|
|
State |
|
DL |
|
|
CDL |
||||||||||||||||||
|
Date |
|
DD |
|
YYYY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
|
N |
|
|
Y |
N |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
MM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Safety Equip. Used |
|
|
|
|
Air Bag |
Ejected |
|
Date of Death |
|
|
|
Injury |
Type |
|
EMS |
|
Transport |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
|
YYYY |
|
|
|
|
|
|
|
|
Y |
|
|
|
|
N |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Summons |
|
|
|
|
Offenses |
Charged |
to Driver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Issued As |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Result of Crash |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
VEHICLE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Vehicle Owner ’s Name (Last, First, Middle) |
|
|
|
|
|
|
|
|
|
|
|
|
Same as Driver |
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Address (Street and Number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
ZIP |
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Vehicle Year |
|
|
Vehicle Make |
|
Vehicle Model |
|
|
|
|
Disabled |
|
CMV |
|
|
Towed |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
Vehicle Plate Number |
|
|
|
|
|
|
|
|
State |
Approximate Repair Cost |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
VIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Oversize |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cargo Spill |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Name of Insurance Company (not agent) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Override |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Underride |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
Speed Before Crash |
|
|
|
Speed Limit |
Maximum Safe Speed |
Under |
|
ALL Passengers Age Count |
|
|
Over |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
21 |
|
|
||||||||
|
|
PASSENGER (only if injured or killed) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
|
|
EMS Transport |
|
|
|
Date of Death |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
MM |
|
|
DD |
|
YY |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Position |
Safety |
|
Airbag |
Ejected |
|
Injury Type |
Birthdate |
|
|
|
|
|
|
|
Gender |
|||||||||||||||||||||
|
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
|
YYYY |
|
|
|
M |
F |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
|
|
EMS Transport |
|
|
|
Date of Death |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
MM |
|
|
DD |
|
YY |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Position |
Safety |
|
Airbag |
Ejected |
|
Injury Type |
Birthdate |
|
|
|
|
|
|
|
Gender |
|||||||||||||||||||||
|
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
|
YYYY |
|
|
|
M |
F |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
|
|
EMS Transport |
|
|
|
Date of Death |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
MM |
|
|
DD |
|
YY |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Position |
Safety |
|
Airbag |
Ejected |
|
Injury Type |
Birthdate |
|
|
|
|
|
|
|
Gender |
|||||||||||||||||||||
|
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
|
YYYY |
|
|
|
M |
F |
|||||||||||||
|
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
VEHICLE # |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
DRIVER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Driver Fled Scene |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Driver’s Name (Last, First, Middle) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Address (Street and Number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
ZIP |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Birth |
|
|
|
|
Drivers License Number |
|
|
|
State |
|
|
DL |
|
CDL |
||||||||||
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
Y |
N |
|
MM |
DD |
YYYY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Safety Equip. Used |
|
Air |
Bag |
Ejected |
Date of Death |
|
|
Injury Type |
|
EMS |
Transport |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
MM |
DD |
|
YYY |
|
|
|
|
|
Y |
|
N |
|
|||
|
Summons |
|
|
|
Offenses |
Charged |
to Driver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Issued As |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Result of Crash |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vehicle Owner ’s Name (Last, First, Middle) |
|
|
|
|
|
|
|
|
|
Same as Driver |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Address (Street and Number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
ZIP |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Vehicle Year |
Vehicle Make |
|
Vehicle Model |
|
|
|
|
Disabled |
CMV |
|
Towed |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vehicle Plate Number |
|
|
|
|
|
|
|
|
|
State |
|
Approximate Repair Cost |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Oversize |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cargo Spill |
|||
|
Name of Insurance Company (not agent) |
|
|
|
|
|
|
|
|
|
|
|
|
Override |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Underride |
|||
|
Speed Before Crash |
|
Speed Limit |
Maximum Safe Speed |
Under |
ALL Passengers Age Count |
Over |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
21 |
|
|
||||
|
PASSENGER (only if injured or killed) |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
EMS Transport |
Date of Death |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
MM |
DD |
YY |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
|
|
Birthdate |
|
|
|
|
Gender |
||||||||||||
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
||||
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
YYYY |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
EMS Transport |
Date of Death |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
MM |
DD |
YY |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
|
|
Birthdate |
|
|
|
|
Gender |
||||||||||||
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
||||
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
YYYY |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
EMS Transport |
Date of Death |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
MM |
DD |
YY |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
|
|
Birthdate |
|
|
|
|
Gender |
||||||||||||
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
||||
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
YYYY |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Codes
8
|
|
1 |
|
|
2 |
|
|
3 |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
5 |
|
|
6 |
|
|||
8 |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
||
POSITION IN/ON VEHICLE
1.Driver
7.Cargo Area
8.Riding/Hanging
8On Outside
SAFETY EQUIPMENT USED
1.Lap Belt Only
2.Shoulder Belt Only
3.Lap and Shoulder Belt
4.Child Restraint
5.Helmet
6.Other
7.Booster Seat
8.No Restraint Used
9.Not Applicable
AIRBAG
1.Deployed – Front
2.Not Deployed
3.Unavailable/Not Applicable
4.Keyed Off
5.Unknown
6.Deployed – Side
7.Deployed – Other (Knee, Air Belt, etc.)
8.Deployed – Combination
EJECTED FROM VEHICLE
1.Not Ejected
2.Partially Ejected
3.Totally Ejected
SUMMONS ISSUED AS A RESULT OF CRASH
1.Yes
2.No
3.Pending
INJURY TYPE
1.Dead
2.Serious Injury
3.Minor/Possible Injury
4.No Apparent Injury
6. No Injury (driver only)
Investigating Officer
Badge/Code Number
Agency/Department Name and Code
Reviewing Officer
Report File Date
Officer Initials________ Badge # __________ |
Commonwealth of Virginia • Department of Motor Vehicles |
FR300P (Rev 1/12) |
Revised Report |
Police Crash Report |
Page _______ of _______ |
|
CRASH
Crash MM DD YYYY Date
MILITARY Time (24 hr clock)
County of Crash
City of Town of
Local Case Number
DRIVER INFORMATION
VEHICLE INFORMATION
Veh |
|
Veh |
|
Veh |
|
Veh |
|
|
|
|
|
|
|
Veh Veh
Veh Veh |
N/A N/A Driver’s Action |
P1 |
1. No Improper Action
2. Exceeded Speed Limit
3. Exceeded Safe Speed
But Not Speed Limit
4. Overtaking On Hill
5. Overtaking On Curve
6. Overtaking at Intersection
7. Improper Passing of School Bus
8. Cutting In
9. Other Improper Passing
10. Wrong Side of Road – Not Overtaking
11. Did Not Have
12. Following Too Close
13. Fail to Signal or Improper Signal
14. Improper Turn – Wide Right Turn
15. Improper Turn –
Cut Corner on Left Turn
16. Improper Turn From Wrong Lane
17. Other Improper Turn
18. Improper Backing
19. Improper Start From Parked Position
20. Disregarded Officer or Flagger
21. Disregarded Traffic Signal
22. Disregarded Stop or Yield Sign
23. Driver Distraction
24. Fail to Stop at Through High way – No Sign
25. Drive Through Work Zone
26. Fail to Set Out Flares or Flags
27. Fail to Dim Headlights
28. Driving Without Lights
29. Improper Parking Location
30. Avoiding Pedestrian
31. Avoiding Other Vehicle
32. Avoiding Animal
33. Crowded Off Highway
34. Hit and Run
35. Car Ran Away – No Driver
36. Blinded by Headlights
37. Other
38. Avoiding Object in Roadway
39. Eluding Police
40. Fail to Maintain Proper Control
41. Improper Passing
42. Improper or Unsafe Lane Change
43. Over Correction
N/A N/A Condition of |
Driver |
P2 |
Contributing |
to the |
Crash |
|
|
|
1. No Defects
2. Eyesight Defective
3. Hearing Defective
4. Other Body Defects
5. Illness
6. Fatigued
7. Apparently Asleep
8. Other
9. Unknown
N/A N/A Driver Vision Obscured P3
1. Not Obscured
2. Rain, Snow, etc. on Windshield
3. Windshield Otherwise Ob scured
4. Vision Obscured by Load on Vehicle
5. Trees, Crops, etc.
6. Building
7. Embankment
8. Sign or Signboard
9. Hillcrest
10. Parked Vehicle(s)
11. Moving Vehicle(s)
12. Sun or Headlight Glare
13. Other
14. Blind Spot
15. Smoke/Dust
16. Stopped Vehicle(s)
N/A N/A Type of Driver |
P4 |
Distractions |
|
1. Looking at Roadside Incident
2. Driver Fatigue
3. Looking at Scenery
4. Passenger(s)
5. Radio/CD, etc.
6. Cell Phone
7. Eyes Not on Road
8. Daydreaming
9. Eating/Drinking
10. Adjusting Vehicle Controls
11. Other
12. Navigation Device
13. Texting
14. No Driver Distraction
N/A N/A Drinking |
P5 |
1. Had Not Been Drinking
2. Drinking – Obviously Drunk
3. Drinking – Ability Im paired
4. Drinking – Ability Not Impaired
5. Drinking – Not Known Whether Impaired
6. Unknown
N/A N/A Method of Alcohol P6
Determination (by police)
1. Blood
2. Breath
3. Refused
4. No Test
N/A N/A Drug Use |
P7 |
1. Yes
2. No
3. Unknown
N/A |
N/A |
Vehicle Maneuver |
V1 |
||
|
|
1. |
Going Straight Ahead |
|
|
|
|
2. |
Making Right Turn |
|
|
|
|
3. |
Making Left Turn |
|
|
|
|
4. Making |
|
||
|
|
5. |
Slowing or Stopping |
|
|
|
|
6. |
Merging Into Traffic Lane |
|
|
|
|
7. |
Starting From Parked Position |
|
|
|
|
8. |
Stopped in Traffic Lane |
|
|
|
|
9. |
Ran Off Road – Right |
|
|
|
|
10. |
Ran Off Road – Left |
|
|
|
|
11. |
Parked |
|
|
|
|
12. |
Backing |
|
|
|
|
13. |
Passing |
|
|
|
|
14. Changing Lanes |
|
||
|
|
15. |
Other |
|
|
|
|
16. |
Entering Street From arking Lot |
||
N/A |
N/A |
Skidding Tire/Mark |
V2 |
||
1. Before Application of Brakes
2. After Application of Brakes
3. Before and After Application of Brakes
4. No Visible Skid Mark/Tire Mark
N/A N/A Vehicle Body Type |
V3 |
1. Passenger car
2. Truck –
3. Van
4. Truck – Single Unit Truck
7. Motor Home, Recreational Vehicle
8. Special Vehicle – Oversized Vehicle/Earthmover/Road Equipment
9. Bicycle
10. Moped
11. Motorcycle
12. Emergency Vehicle (Regardless of Vehicle Type)
13. Bus – School Bus
14. Bus – City Transit Bus/Privately Owned Church Bus
15. Bus – Commercial Bus
16. Other (Scooter,
18. Special Vehicle – Farm Machinery
19. Special Vehicle – ATV
21. Special Vehicle –
22. Truck – Sport Utility Vehicle (SUV)
23. Truck – Single Unit Truck (3 Axles or More)
25. Truck – Truck Tractor
N/A N/A Vehicle Damage |
V4 |
1. Unknown
2. No damage
3. Overturned
4. Motor
5. Undercarriage
6. Totaled
7. Fire
8. Other
N/A N/A Vehicle Condition |
V5 |
1. No Defects
2. Lights Defective
3. Brakes Defective
4. Steering Defective
5. Puncture/Blowout
6. Worn or Slick Tires
7. Motor Trouble
8. Chains In Use
9. Other
10. Vehicle Altered
11. Mirrors Defective
12. Power Train Defective
13. Suspension Defective
14. Windows/Windshield Defective
15. Wipers Defective
16. Wheels Defective
17. Exhaust System
N/A |
N/A |
Special Function |
V6 |
|
|
|
Motor Vehicle |
|
|
|
|
1. |
No Special Function |
|
|
|
2. |
Taxi |
|
|
|
3. School Bus (Public or Private) |
||
|
|
4. |
Transit Bus |
|
|
|
5. |
Intercity Bus |
|
N/A |
N/A |
6. Charter Bus |
|
|
|
|
7. Other Bus |
|
|
|
|
8. |
Military |
|
|
|
9. |
Police |
|
|
|
10. Ambulance |
|
|
|
|
11. Fire Truck |
|
|
|
|
12. Tow Truck |
|
|
|
|
13. Maintenance |
|
|
|
|
14. Unknown |
|
|
N/A |
N/A |
EMV in service |
V7 |
|
|
|
1. |
Yes |
|
|
|
2. No |
|
|
N/A |
N/A |
Truck Cover |
V8 |
|
|
|
1. |
Yes |
|
2. No
Officer Initials________ Badge # __________ |
Commonwealth of Virginia |
• |
Department of Motor Vehicles |
FR300P (Rev 1/12) |
|
|
|
|
Revised Report |
Police |
Crash Report |
Page _______ of _______ |
|
|
CRASH
Crash MM DD YYYY Date
MILITARY Time (24 hr clock)
County of Crash
City of Town of
Local Case Number
CRASH INFORMATION
Location |
of First Harmful |
C1 |
Event in |
Relation to Roadway |
|
1. On Roadway
2. Shoulder
3. Median
4. Roadside
5. Gore
6. Separator
7. In Parking Lane or Zone
8. Off Roadway, Location Unknown
9. Outside
Weather Condition |
C2 |
1. No Adverse Condition
(Clear/Cloudy)
3. Fog
4. Mist
5. Rain
6. Snow
7. Sleet/Hail
8. Smoke/Dust
9. Other
10. Blowing Sand, Soil,
Dirt, or Snow
11. Severe Crosswinds
Light Conditions |
C3 |
|
|
1. Dawn
2. Daylight
3. Dusk
4. Darkness
5. Darkness
6. Darkness
Road Lighting
7. Unknown
Traffic Control |
C4 |
Device |
|
|
|
1. Yes – Working
2. Yes – Working and Obscured
3. Yes – Not Working
4. Yes – Not Working and Obscured
5. Yes – Missing
6. No Traffic Control Device Present
Traffic Control Type |
C5 |
|
|
1. No Traffic Control
2. Officer or Flagger
3. Traffic Signal
4. Stop Sign
5. Slow or Warning Sign
6. Traffic Lanes Marked
7. No Passing Lines
8. Yield Sign
9. One Way Road or Street
10. Railroad Crossing With
Markings and Signs
11. Railroad Crossing With Signals
12. Railroad Crossing With Gate and Signals
13. Other
14. Pedestrian Crosswalk
15. Reduced Speed – School Zone
16. Reduced Speed – Work Zone
17. Highway Safety Corridor
Roadway Alignment |
C6 |
|
|
1. Straight – Level
2. Curve – Level
3. Grade – Straight
4. Grade – Curve
5. Hillcrest – Straight
6. Hillcrest – Curve
7. Dip – Straight
8. Dip – Curve
9. Other
10. On/Off Ramp
Roadway Surface Condition C7
1. Dry
2. Wet
3. Snowy
4. Icy
5. Muddy
6. Oil/Other Fluids
7. Other
8. Natural Debris
9. Water (Standing, Moving)
10. Slush
11. Sand, Dirt, Gravel
Roadway Surface Type |
C8 |
|
|
1. Concrete
2. Blacktop, Asphalt, Bituminous
3. Brick or Block
4. Slag, Gravel, Stone
5. Dirt
6. Other
Roadway Description |
C9 |
|
|
1.
2.
Unprotected Median
3.
Median Barrier
4.
5. Unknown
Roadway Defects |
C10 |
|
|
1. No Defects
2. Holes, Ruts, Bumps
3. Soft or Low Shoulder
4. Under Repair
5. Loose Material
6. Restricted Width
7. Slick Pavement
8. Roadway Obstructed
9. Other
10. Edge Pavement Drop Off
Relation to Roadway |
C11 |
Interchange Area: |
|
1.
2. Acceleration/Deceleration Lanes
3. Gore Area (Between Ramp and Highway Edgelines)
4. Collector/Distributor Road
5. On Entrance/Exit Ramp
6. Intersection at end of Ramp
7. Other location not listed above within an interchange area (median, shoulder and roadside)
Intersection Area:
8.
9. Within Intersection
10.
11.
Other Location:
12. Crossover Related
13. Driveway,
14. Railway Grade Crossing
15. Other Crossing (Crossings for Bikes, School, etc.)
Intersection Type |
C12 |
|
|
1. Not at Intersection
2. Two Approaches
3. Three Approaches
4. Four Approaches
5.
6. Roundabout
Work Zone |
C13 |
1. Yes |
|
2. No |
|
|
|
|
|
Work Zone |
C14 |
Workers Present |
|
1. With Law Enforcement |
|
2. With No Law Enforcement |
|
3. No Workers Present |
|
|
|
|
|
Work Zone Location |
C15 |
|
|
1. Advance Warning Area
2. Transition Area
3. Activity Area
4. Termination Area
Work Zone Type |
C16 |
|
|
1. Lane Closure
2. Lane Shift/Crossover
3. Work on Shoulder or Median
4. Intermittent or Moving Work
5. Other
School Zone |
C17 |
|
1. |
Yes |
|
2. |
Yes - With School Activity |
|
3. No |
|
|
|
|
|
|
|
|
Type of Collision |
C18 |
|
|
|
|
1. Rear End
2. Angle
3. Head On
4. Sideswipe – Same Direction
5. Sideswipe – Opposite Direction
6. Fixed Object in Road
7. Train
8.
9. Fixed Object – Off Road
10. Deer
11. Other Animal
12. Pedestrian
13. Bicyclist
14. Motorcyclist
15. Backed Into
16. Other
Officer Initials________ Badge # __________ |
Commonwealth of Virginia |
• |
Department of Motor Vehicles |
FR300P (Rev 1/12) |
Revised Report |
Police |
Crash Report |
Page _______ of _______ |
|
|
CRASH
Crash MM DD YYYY Date
MILITARY Time (24 hr clock)
County of Crash
City of Town of
Local Case Number
VEHICLE # 

Fill In Impact Area(s). Initial Impact. 
|
12 |
|
11 |
|
1 |
10 |
|
2 |
9 |
13 |
3 |
8 |
|
4 |
7 |
|
5 |
|
6 |
|
Veh Dir of Travel
VEHICLE # 

Fill In Impact Area(s). Initial Impact. 
|
12 |
|
11 |
|
1 |
10 |
|
2 |
9 |
13 |
3 |
8 |
|
4 |
7 |
|
5 |
|
6 |
|
Veh Dir of Travel
CRASH DIAGRAM
Indicate North by Arrow
VEHICLE # 

Fill In Impact Area(s). Initial Impact. 
|
12 |
|
11 |
|
1 |
10 |
|
2 |
9 |
13 |
3 |
8 |
|
4 |
7 |
|
5 |
|
6 |
|
Veh Dir of Travel
VEHICLE # 

Fill In Impact Area(s). Initial Impact. 
|
12 |
|
11 |
|
1 |
10 |
|
2 |
9 |
13 |
3 |
8 |
|
4 |
7 |
|
5 |
|
6 |
|
Veh Dir of Travel
DAMAGE TO PROPERTY OTHER THAN VEHICLES
Approx. Repair Cost
Object Struck (Tree, Fence, etc.)
Property Owners Name (Last, First, iddle)
Address (Street and Number)
VDOT Property
Yes No
CRASH DESCRIPTION
CRASH EVENTS
Vehicle # |
First Event |
Second Event |
Third Event |
Fourth Event |
Most Harmful Event |
|
|
|
|
|
|
|
|
|
|
|
|
Vehicle # |
First Event |
Second Event |
Third Event |
Fourth Event |
Most Harmful Event |
|
|
|
|
|
|
Vehicle # |
First Event |
Second Event |
Third Event |
Fourth Event |
Most Harmful Event |
|
|
|
|
|
|
|
|
|
|
|
|
Vehicle # |
First Event |
Second Event |
Third Event |
Fourth Event |
Most Harmful Event |
|
|
|
|
|
|
First Harmful Event of Entire Crash that Results in First Injury or Damage.
COLLISION WITH FIXED OBJECT
1. Bank Or Ledge |
10. Other |
||
2. |
Trees |
11. |
Jersey Wall |
3. |
Utility Pole |
12. |
Building/Structure |
4. |
Fence Or Post |
13. |
Curb |
5. |
Guard Rail |
14. |
Ditch |
6. |
Parked Vehicle |
15. |
Other Fixed Object |
7. |
Tunnel, Bridge, Underpass, |
16. |
Other Traffic Barrier |
|
Culvert, etc. |
17. |
Traffic Sign Support |
8. |
Sign, Traffic Signal |
18. |
Mailbox |
9. Impact Cushioning Device
COLLISION WITH PERSON, MOTOR VEHICLE |
|
|
||||
OR |
24. Work Zone |
28. Ran Off Road |
35. Cross Median |
|||
19. |
Pedestrian |
29. |
Jack Knife |
36. |
Cross Centerline |
|
20. |
Motor Vehicle In Transport |
Maintenance Equipment |
30. |
Overturn (Rollover) |
37. |
Equipment Failure (Tire, etc) |
21. |
Train |
25. Other Movable Object |
31. |
Downhill Runaway |
38. |
Immersion |
22. |
Bicycle |
26. Unknown Movable Object |
32. |
Cargo Loss or Shift |
39. |
Fell/Jumped From Vehicle |
23. |
Animal |
27. Other |
33. |
Explosion or Fire |
40. |
Thrown or Falling Object |
|
|
|
34. |
Separation of Units |
41. |
|
|
|
|
|
|
42. |
Other |
Officer Initials________ Badge # __________ |
Commonwealth of Virginia • Department of Motor Vehicles |
FR300P (Rev 1/12) |
Revised Report |
Police Crash Report |
Page _______ of _______ |
|
CRASH
Crash MM DD YYYY Date
MILITARY Time (24 hr clock)
County of Crash
City of Town of
Local Case Number
COMMERCIAL MOTOR VEHICLE SECTION
This form is being completed because the vehicle is:
A Truck or Truck Combination Rating Greater Than 10,000 lbs. (GVWR/GCWR)
Any Motor Vehicle That Seats
9 or More People, Including the Driver
A Vehicle of Any Type with a Hazardous Materials Placard Regardless of Weight
AND The crash resulted in:
A fatality: any person(s) killed in or outside of any |
|
|
|
An injury: any person(s) injured as a |
|
|
|
|
|
|
A |
|
|||||||||||||||
vehicle (truck, bus, car, etc.) involved in the crash or |
|
OR |
result of the crash who immediately |
OR |
|
|
bus, car, etc.) disabled as a result of the |
|
|||||||||||||||||||
who dies within 30 days of the crash as a result of |
|
|
|
receives medical treatment away from |
|
|
crash and transported away from the |
|
|||||||||||||||||||
an injury sustained in the crash |
|
|
|
|
the crash scene |
|
|
|
|
|
|
|
scene by a tow truck or other vehicle |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Vehicle Configuration |
|
V10 |
|
Cargo Body Type |
|
|
V11 |
|
|
License P8 |
|
Commercial |
|
P9 |
|||||||||||||
1. |
Passenger Car (Only if Vehicle Has Hazardous Materials Placard) |
|
1. Bus (Seats |
10. Grain/Chips/Gravel |
|
|
Class |
|
|
Endorsement |
|
||||||||||||||||
2. |
Light Truck (Only if Vehicle Has Hazardous Materials Placard) |
|
|
|
Including Driver) |
11. |
|
|
|
Class A |
|
|
|
|
|||||||||||||
3. |
Bus (Seats |
|
|
|
2. Bus (Seats For 16 People or |
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
12. Vehicle Towing Another |
|
|
|
Class B |
|
|
|
|||||||||||||||||
4. |
Bus (Seats for 16 People or More, Including Driver) |
|
|
|
More, Including Driver) |
|
|
|
|
|
|
||||||||||||||||
|
|
|
Motor Vehicle |
|
|
|
Class C |
|
|
|
|
||||||||||||||||
|
|
|
3. Van/Enclosed Box |
|
|
|
|
|
|
|
|||||||||||||||||
5. |
Single Unit Truck (2 Axles, 6 Tires) |
|
|
|
|
13. Intermodel Container |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
Class DRL |
|
|
|
|||||||||||||||||
|
|
|
|
4. Cargo Tank |
|
|
|
|
|
|
|||||||||||||||||
6. |
Single Unit Truck (3 or More Axles) |
|
|
|
Chassis |
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
(regular |
|
|
|
Placarded for |
|
||||||||||||||||
|
|
|
5. Flatbed |
14. Logging |
|
|
|
|
|
|
|
||||||||||||||||
7. |
Truck Trailer(s) |
|
|
|
|
|
|
drivers |
|
|
|
Hazardous Materials |
|||||||||||||||
8. Truck Tractor (Bobtail) |
|
|
|
|
6. Dump |
15. ther Cargo Body |
|
|
|
license) |
|
|
|
||||||||||||||
|
|
|
|
|
|
|
Class M |
|
|
||||||||||||||||||
9. |
|
|
|
|
7. Concrete Mixer |
(Not Listed Above) |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
8. Auto Transporter |
16. Not Applicable/ |
|
|
|
|
|
|
|
|
|
|||||||||||||
10. Tractor/Doubles (Two Trailers) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
11. Other Truck Greater Than 10,000 lbs. (Not Listed Above) |
|
|
|
9. Garbage/Refuse |
No |
argo Body |
|
|
GVWR/ V12 |
|
|
1. 10,000 lbs. or Less |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GCWR |
|
|
|
2. |
|
||
Hazardous Material |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. Greater Than 26,000 lbs. |
|||||||||||
Hazardous Material Placard: Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
HM |
|
|
|
|
|
|
|
HM Placard Name |
|
|
|
|
|
HM Class |
|
|
|
|
|
HM Cargo Present |
|
HM Cargo Released |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
Y |
N |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carrier |
Identification |
|
|
|
|
|
|
|
|||
|
Commercial Motor Carrier Name |
|
|
|
Address (P.O. Box if No Street Address) |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carrier’s ID |
Number |
State (Intrastate Only) |
City |
|
State |
Zip |
|||||
|
US DOT# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. Interstate Carrier
2. Intrastate Carrier
3. Not in
VEHICLE #
Vehicle Configuration |
V10 |
|
Cargo Body Type |
|
|
V11 |
|
|
License |
P8 |
|
Commercial |
|
P9 |
||||||||||
1. |
Passenger Car (Only if Vehicle Has Hazardous Materials Placard) |
|
1. Bus (Seats |
10. Grain/Chips/Gravel |
|
|
Class |
|
|
Endorsement |
|
|||||||||||||
2. |
Light Truck (Only if Vehicle Has Hazardous Materials Placard) |
|
Including Driver) |
11. |
|
|
|
Class A |
|
|
|
|
||||||||||||
3. |
Bus (Seats |
|
2. Bus (Seats For 16 People or |
|
|
|
|
|
|
|
||||||||||||||
|
12. Vehicle Towing Another |
|
|
|
Class B |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
More, Including Driver) |
|
|
|
|
|
|
||||||||
4. |
Bus (Seats for 16 People or More, Including Driver) |
|
Motor Vehicle |
|
|
|
Class C |
|
|
|
|
|||||||||||||
|
3. Van/Enclosed Box |
|
|
|
|
|
|
|
||||||||||||||||
5. |
Single Unit Truck (2 Axles, 6 Tires) |
|
|
|
13. Intermodel Container |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
Class DRL |
|
|
|
|||||||||||||||
|
|
|
4. Cargo Tank |
|
|
|
|
|
|
|||||||||||||||
6. |
Single Unit Truck (3 or More Axles) |
|
Chassis |
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
(regular |
|
|
|
Placarded for |
|
|||||||||||||||
|
5. Flatbed |
14. Logging |
|
|
|
|
|
|
|
|||||||||||||||
7. |
Truck Trailer(s) |
|
|
|
|
drivers |
|
|
|
Hazardous Materials |
||||||||||||||
|
6. Dump |
|
|
|
|
|
|
|
license) |
|
|
|
||||||||||||
8. |
Truck Tractor (Bobtail) |
|
|
|
15. Other Cargo Body |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
Class M |
|
|
|
|||||||||||||||
|
|
|
7. Concrete Mixer |
(Not Listed Above) |
|
|
|
|
|
|
||||||||||||||
9. |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
8. Auto Transporter |
16. Not Applicable/ |
|
|
|
|
|
|
|
|
|
|||||||||||
10. Tractor/Doubles (Two Trailers) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
9. Garbage/Refuse |
No Cargo Body |
|
|
GVWR/ V12 |
|
|
1. 10,000 lbs. or Less |
|
|||||||||||||
11. Other Truck Greater Than 10,000 lbs. (Not Listed Above) |
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GCWR |
|
|
|
2. |
|
||
Hazardous Material |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. Greater Than 26,000 lbs. |
|||||||||
Hazardous Material Placard: Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
HM |
|
|
|
|
|
HM Placard Name |
|
|
|
|
HM Class |
|
|
|
|
|
HM Cargo Present |
|
HM Cargo Released |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
Y |
N |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carrier |
Identification |
|
|
|
|
|
|||
|
Commercial Motor Carrier Name |
|
Address (P.O. Box if No Street Address) |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Carrier’s ID |
Number |
State (Intrastate Only) |
City |
|
State |
Zip |
|||
|
US DOT# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. Interstate Carrier
2. Intrastate Carrier
3. Not in
Officer Initials________ Badge # __________ |
Commonwealth of Virginia • Department of Motor Vehicles |
FR300P (Rev 1/12) |
Revised Report |
Police Crash Report |
Page _______ of _______ |
|
CRASH
Crash MM DD YYYY Date
MILITARY Time (24 hr clock)
County of Crash
City of Town of
Local Case Number
|
PEDESTRIAN # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Injured |
Name of Injured (Last, First, Middle) |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address (Street and Number) |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
State |
|
ZIP |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Driver’s License # |
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Gender |
|
EMS Transport |
Injury Type |
Birthdate |
|
|
|
Date of Death |
|
|
|||||||
|
M |
F |
|
|
|
|
|
DD |
|
YYYY |
MM |
|
DD |
|
YYYY |
|||
|
|
Y |
N |
|
MM |
|
|
|
|
|||||||||
|
PEDESTRIAN # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Injured |
Name of Injured (Last, First, Middle) |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address (Street and Number) |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
State |
|
ZIP |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Driver’s License # |
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Gender |
|
EMS Transport |
Injury Type |
Birthdate |
|
|
|
Date of Death |
|
|
|||||||
|
M |
F |
|
|
|
|
|
|
DD |
|
YYYY |
MM |
|
DD |
|
YYYY |
||
|
|
Y |
N |
|
MM |
|
|
|
|
|||||||||
Ped # |
|
Ped # |
|
Ped # |
|
Ped # |
|
Ped # |
|
Ped # |
|
Ped # |
|
Ped # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N/A |
N/A |
Pedestrian Actions |
P10 |
|
|
|
1. |
Crossing At Intersection |
11. Hitching On Vehicle |
|
|
|
With Signal |
12. Walking In Roadway |
|
|
2. |
Crossing At Intersection |
|
|
|
With Traffic – Sidewalks |
||
|
|
|
Against Signal |
Available |
|
|
3. |
Crossing At Intersection |
13. Walking In Roadway |
|
|
|
No Signal |
With Traffic – Sidewalks |
|
|
4. |
Crossing At Intersection |
Not Available |
|
|
|
Diagonally |
14. Walking In Roadway |
|
|
5. |
Crossing Not At |
Against Traffic |
|
|
|
Intersection – Rural |
– Sidewalks Available |
|
|
6. Crossing Not At |
15. Walking In Roadway |
|
|
|
|
Intersection – Urban |
Against Traffic – Side |
|
|
7. Coming From Behind |
Walks Not Available |
|
|
|
16. Working In Roadway |
||
|
|
|
Parked Cars |
|
|
|
8. Getting Off Or On |
17. Standing In Roadway |
|
|
|
|
School Bus |
18. Lying In Roadway |
|
|
9. Playing In Roadway |
19. Not In Roadway |
|
|
|
10. Getting Off Or On |
20. Other |
|
|
|
|
Another Vehicle |
|
N/A N/A Pedestrian Drinking P11
1. Had Not Been Drinking
2.
3. Drinking
4. Drinking
5. Drinking
Whether Impaired
N/A N/A Condition of |
P12 |
Pedestrian |
|
ontributing |
to |
the rash |
|
|
|
1. No Defects
2. Eyesight Defective
3. Hearing Defective
4. Other Body Defects
5. Illness
6. Fatigued
7. Apparently Asleep
8. Other
N/A |
N/A |
Method of |
P13 |
|
|
|
Alcohol |
|
|
|
|
Determination |
|
|
|
|
by Police |
|
|
|
|
1. |
Blood |
|
|
|
2. |
Breath |
|
|
|
3. |
Refused |
|
|
|
4. |
No Test |
|
N/A |
N/A |
Pedestrian Drug Use P14 |
||
|
|
1. |
Yes |
|
|
|
2. No |
|
|
|
|
3. Unknown |
|
|
N/A |
N/A |
Pedestrian Wear |
P15 |
|
|
|
Reflective Clothing |
|
|
|
|
1. |
Yes |
|
2. No
Use sections below for additional passengers.
VEHICLE #
PASSENGER (only if injured or killed)
|
Name of Injured |
(Last, First, Middle) |
|
|
EMS Transport |
|
Date of Death |
||||||||
|
|
|
|
|
|
Y |
N |
|
MM |
|
DD |
|
YY |
||
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
Birthdate |
|
|
|
Gender |
|||||
|
In/On |
Equip |
|
|
|
MM |
|
DD |
|
YYYY |
|
M |
|
F |
|
|
|
|
|
|
|
|
|
||||||||
|
Vehicle |
Used |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
||||||||
|
Name of Injured |
(Last, First, Middle) |
|
|
EMS Transport |
|
Date of Death |
||||||||
|
|
|
|
|
|
Y |
N |
|
MM |
|
DD |
|
YY |
||
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
Birthdate |
|
|
|
Gender |
|||||
|
In/On |
Equip |
|
|
|
MM |
|
DD |
|
YYYY |
|
M |
|
F |
|
|
|
|
|
|
|
|
|
||||||||
|
Vehicle |
Used |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
||||||||
|
Name of Injured |
(Last, First, Middle) |
|
|
EMS Transport |
|
Date of Death |
||||||||
|
|
|
|
|
|
Y |
N |
|
MM |
|
DD |
|
YY |
||
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
Birthdate |
|
|
|
Gender |
|||||
|
In/On |
Equip |
|
|
|
MM |
|
DD |
|
YYYY |
|
M |
|
F |
|
|
|
|
|
|
|
|
|
||||||||
|
Vehicle |
Used |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||||||
VEHICLE #
PASSENGER (only if injured or killed)
|
Name of Injured |
(Last, First, Middle) |
|
|
EMS Transport |
Date of Death |
||||||||
|
Injured |
|
|
|
|
|
Y |
N |
MM |
|
DD |
|
YY |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
Birthdate |
|
|
|
Gender |
||||
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
M |
|
F |
|
Vehicle |
Used |
|
|
|
MM |
|
DD |
YYYY |
|
|
|||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Injured |
(Last, First, Middle) |
|
|
EMS Transport |
Date of Death |
||||||||
|
InjuredPosition |
|
|
|
|
|
Y |
N |
MM |
|
DD |
|
YY |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Safety |
Airbag |
Ejected |
Injury Type |
Birthdate |
|
|
|
Gender |
|||||
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
M |
|
F |
|
Vehicle |
Used |
|
|
|
MM |
|
DD |
YYYY |
|
|
|||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Injured |
(Last, First, Middle) |
|
|
EMS Transport |
Date of Death |
||||||||
|
|
|
|
|
|
|
Y |
N |
MM |
|
DD |
|
YY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
Birthdate |
YYYY |
|
Gender |
|||||
|
InjuredVehicle |
Used |
|
|
|
MM |
|
DD |
|
|
|
|
||
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
M |
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Codes
8
|
|
1 |
|
|
2 |
|
|
3 |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
6 |
|
|||||
|
|
|
5 |
|
|
|
|||||
8 |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
7 |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|||
POSITION IN/ON VEHICLE
1.Driver
7.Cargo Area
8.Riding/Hanging
8On Outside
SAFETY EQUIPMENT USED
1.Lap Belt Only
2.Shoulder Belt Only
3.Lap and Shoulder Belt
4.Child Restraint
5.Helmet
6.Other
7.Booster Seat
8.No Restraint Used
9.Not Applicable
AIRBAG
1.Deployed – Front
2.Not Deployed
3.Unavailable/Not Applicable
4.Keyed Off
5.Unknown
6.Deployed – Side
7.Deployed – Other (Knee, Air Belt, etc.)
8.Deployed – Combination
EJECTED FROM VEHICLE
1.Not Ejected
2.Partially Ejected
3.Totally Ejected
SUMMONS ISSUED AS A RESULT OF CRASH
1.Yes
2.No
3.Pending
INJURY TYPE
1.Dead
2.Serious Injury
3.Minor/Possible Injury
4.No Apparent Injury
Form Properties
| # | Fact | Details |
|---|---|---|
| 1 | Form Identification | The form is identified as FR300P, revised as of January 2012. |
| 2 | Purpose | It is used by the Virginia Police to report motor vehicle crashes. |
| 3 | Requirement | Completion is necessary for crashes that involve injury, death, or significant property damage. |
| 4 | Data Recorded | Includes details about the crash, driver, vehicle, passengers, and any commercial vehicle specifics. |
| 5 | GPS Information | Crash location is recorded using GPS coordinates for precise location mapping. |
| 6 | Critical Timestamps | Documents the date and military time of the crash, enhancing report accuracy. |
| 7 | Governing Law | Governed under the Virginia state laws related to road safety and vehicle operation. |
Steps to Filling Out Virginia Police Crash Report
When there's been a vehicle crash in Virginia, it's essential to accurately complete the Virginia Police Crash Report form. This document is crucial for law enforcement to document the details of the incident thoroughly. Presenting facts clearly can significantly impact the investigation and any subsequent insurance claims or legal actions. The process might seem daunting, but knowing what information is required can simplify it. Follow these step-by-step instructions to ensure the form is filled out correctly.
- Start with the crash information: Enter the date (MM DD YYYY), day of the week, and military time when the crash occurred. Include GPS coordinates if available.
- Fill in the location details: Specify the county, city or town where the crash happened, and give a precise location using the available fields for route/street, landmarks, and if applicable, railroad crossing ID.
- Record the crash specifics: Indicate the number of vehicles involved, the crash's nature (at an intersection, specific miles or feet from a notable location), and if there were any non-vehicle property damage.
- Detail each vehicle involved: For every vehicle in the crash, document the driver's information (name, address, gender, birth date, driver's license number, and state), vehicle details (owner's name, year, make, model, license plate number, insurance information), and any relevant crash details (safety equipment used, airbag status, ejections, injuries, fatalities).
- Note passenger information: If there were any passengers injured or killed in the crash, include their names, safety equipment used, airbag status, injuries, or fatalities.
- Document crash dynamics: Fill in details regarding the initial impact, vehicle direction of travel, and for commercial vehicles, additional information regarding the vehicle configuration, cargo type, and hazardous material details if applicable.
- Include crash event descriptions: Use the codes provided to describe the crash events for each vehicle involved. Detail the first harmful event and any subsequent events leading to injuries or damage.
- Provide investigator information: The officer investigating the crash should include their badge/code number, agency/department name and code, and file date.
- Complete the commercial motor vehicle section: If the crash involved a commercial vehicle, fill out the required sections regarding the vehicle's configuration, cargo body type, commercial license endorsements, hazardous material details, carrier identification, and whether it was an interstate or intrastate carrier.
- Review and finalize the report: Ensure all information is accurate and complete. Check that all involved parties have been accounted for and that the crash details are thoroughly documented.
Once the form is fully completed, it will be reviewed by the designated law enforcement agency to proceed with their investigation. It becomes a vital record for understanding the circumstances surrounding the crash, as well as for insurance and legal purposes. Remember, providing complete and accurate information is key to ensuring the report is as helpful as possible.
FAQ
What is the purpose of the Virginia Police Crash Report form?
The Virginia Police Crash Report form, designated as FR300P, is used by law enforcement officers in the Commonwealth of Virginia to document detailed information about a motor vehicle crash. This report captures a wide array of data, including but not limited to, the date, time, and location of the crash, party demographics (drivers, passengers, vehicle owners), vehicle specifics, crash dynamics, environmental conditions, and the apparent causes of the incident. The information collected is critical for several purposes: it aids in the legal and insurance claim processes, supports law enforcement in crash analysis and prevention strategies, and contributes to road safety research and policy development by identifying patterns and causes of crashes.
Who completes the Virginia Police Crash Report form?
The FR300P form is completed by a law enforcement officer responding to a motor vehicle crash scene. The officer is responsible for conducting an initial investigation, collecting evidence, interviewing witnesses, and documenting the facts surrounding the crash. Based on these findings, the officer fills out the form, detailing all relevant information concerning the crash. It is paramount that the officer provides accurate and comprehensive information to ensure the report serves its intended use effectively.
When is a Virginia Police Crash Report required?
A Police Crash Report in Virginia is typically required in situations where a crash results in bodily injury, death, or significant property damage. Specifically, the law mandates the completion of a crash report if the incident leads to:
- Any person's injury or death as a result of the crash.
- Property damage exceeding a certain threshold, which necessitates the involvement of law enforcement for documentation and reporting purposes.
- The involvement of a commercial motor vehicle, irrespective of the apparent damage or injuries, due to regulatory requirements for reporting incidents involving commercial vehicles.
How can individuals obtain a copy of a completed Virginia Police Crash Report?
Individuals involved in a crash, their legal representatives, or insurance companies may request a copy of the completed Virginia Police Crash Report form. The report is typically available through:
- The local law enforcement agency that responded to and documented the crash. This could be the local police department, sheriff's office, or state police office, depending on the location of the incident.
- The Virginia Department of Motor Vehicles (DMF). Requests can be made in person, by mail, or through the DMV's official website, subject to the submission of required identification and payment of a nominal fee, if applicable.
Common mistakes
Filling out the Virginia Police Crash Report form correctly is crucial for ensuring all details regarding the crash are accurately reported. However, several common mistakes can lead to incomplete or incorrect information being provided. Here are seven such mistakes people often make:
Not providing exact location details: The form requires specific information about the crash location, including the county, city, or town, and the precise route/street. Failing to provide detailed location information, such as the mile marker number or proximity to landmarks, can hinder the accuracy of the report.
Omitting details about the crash conditions: It's essential to accurately document the conditions surrounding the crash, including the weather, lighting, and roadway conditions. Skipping these details or providing incorrect information can affect the understanding of the crash circumstances.
Incorrect vehicle and driver information: Each vehicle involved in the crash needs to have detailed information reported, including the make, model, year, and license plate number. Additionally, driver details such as name, address, driver’s license number, and insurance information must be accurately filled out. Errors or omissions in this area can complicate insurance claims and legal proceedings.
Failing to document injuries or fatalities accurately: The form has specific sections for reporting injuries, fatalities, and the use of safety equipment like seat belts and airbags. Not accurately documenting the type and severity of injuries or fatalities can impact insurance claims and medical treatment for those involved.
Incomplete documentation of the crash events: The form requires a detailed account of the crash events, including the sequence of events and the point of impact. Missing or vague details about how the crash occurred can lead to misunderstandings about fault and liability.
Overlooking details about commercial vehicles: If the crash involved a commercial motor vehicle, additional information is required, such as the vehicle configuration, cargo body type, and whether it was carrying hazardous materials. Neglecting this information can have significant legal and safety implications.
Not using the correct codes for information fields: The form includes codes for various information fields, such as the type of collision, driver actions contributing to the crash, and vehicle maneuvers. Not using these codes correctly can lead to important information being misrepresented or overlooked.
To avoid these mistakes, it's important to carefully review the entire form, double-check all details, and ensure that all relevant sections are completed accurately. This not only facilitates a smoother investigation process but also ensures that all parties involved have the correct information for insurance and legal purposes.
Documents used along the form
When dealing with traffic incidents in Virginia, especially those necessitating a Virginia Police Crash Report, various other documents and forms often supplement these reports for a comprehensive documentation and follow-through. These additional materials serve varied purposes, from insurance claims processing to legal proceedings. Understanding these documents ensures a more navigable aftermath for all parties involved in vehicular incidents.
- Insurance Claim Form: This is a standardized form provided by insurance companies for policyholders to report an accident. It's essential for initiating the process of an insurance claim, detailing the incident, and outlining the damages and injuries, if any.
- Medical Records Release Form: This form authorizes the disclosure of medical records to insurance companies or law firms. It's crucial for substantiating injury claims related to the crash.
- Vehicle Repair Estimates: Professional estimates from auto repair shops that outline the cost of repairing the vehicle damage sustained in the crash. These estimates are vital for insurance claims and legal purposes.
- Witness Statement Form: This document records the accounts of witnesses to the accident. Witness statements can provide additional perspectives on the crash, contributing to the determination of fault.
- Traffic Citation: A document issued by law enforcement if any traffic laws were violated leading to or during the incident. Citations can impact insurance claims and legal liability.
- DMV Accident Report: In Virginia, drivers involved in certain accidents must also file a report with the Department of Motor Vehicles. This is separate from the police report and is necessary for incidents meeting specific criteria set by Virginia law.
- Personal Injury Log: A personally maintained log documenting the injuries sustained, treatment received, and how the injuries have impacted the individual's daily life. This log can be critical in personal injury cases for claiming damages.
Each form and document associated with a Virginia Police Crash Notice plays a specific role in the aftermath of a traffic incident. From initiating an insurance claim to legal proceedings for personal injury, these supplementary documents ensure a thorough and detailed account of the event, aiding all parties involved towards resolution and recovery.
Similar forms
The Virginia Police Crash Report form is similar to other official documents used in documenting vehicular incidents, notably in terms of structure, content, and purpose. Two such documents include the National Highway Traffic Safety Administration's (NHTSA) crash report form and commercial vehicle inspection reports. Each of these documents shares common features with the Virginia Police Crash Report, yet they also embody specific characteristics tailored to their unique reporting requirements.
The National Highway Traffic Safety Administration's (NHTSA) crash report form closely resembles the Virginia Police Crash Report in its comprehensive approach to capturing details about vehicular crashes. Like the Virginia form, the NHTSA's version collects extensive data on the crash scene, involved parties, and vehicular information. Both documents are designed to provide a thorough account of the crash to support investigations and statistical analyses. Key similarities include sections on vehicle and driver information, crash dynamics, and environmental conditions at the time of the crash. However, the NHTSA’s form is utilized for a broader, national data collection effort to inform safety regulations and transportation policies, emphasizing its role in federal safety analysis efforts.
Similarly, commercial vehicle inspection reports share common ground with the Virginia Police Crash Report, particularly in the depth of vehicle-specific information they gather. These inspection reports focus on the condition and compliance of commercial vehicles with safety standards, encompassing details on vehicle parts, cargo, and compliance with federal regulations. While the primary purpose differs—inspection reports aim to prevent incidents by ensuring vehicle safety, as opposed to documenting them post-occurrence—both forms of documentation prioritize detailed, accurate vehicle descriptions. Elements such as vehicle identification number (VIN), cargo type, and safety equipment status are consistently emphasized, showcasing the critical role of vehicle condition in both prevention and analysis of crashes.
Dos and Don'ts
Filling out the Virginia Police Crash Report form accurately is crucial for documenting the incident details and ensures all parties involved have a clear account of the event. Below is a list of dos and don'ts that can help guide you through the process effectively.
Do:
- Ensure all information is legible and written in black ink to prevent mishandlings or misunderstandings of the details provided.
- Double-check the crash date, time (in military format), and location for accuracy to ensure the report correctly reflects the incident specifics.
- Complete every section pertinent to the crash, even those that may seem insignificant, as they may hold crucial details for accurate report documentation.
- Use the correct codes from the provided lists for describing vehicle positions, safety equipment used, and the type of collision to maintain consistency and clarity across reports.
- Include precise descriptions of the crash scene, specifying the direction of travel and impact points on the vehicles involved to aid in the visualization of the incident.
- Report any property damage with accurate estimates and identify the property owner correctly to facilitate potential insurance claims or legal proceedings.
- Detail any injuries sustained during the crash with specific attention to the injury type and the individual's position in or on the vehicle to ensure appropriate medical attention and records.
Don't:
- Leave any section blank; if a section does not apply, indicate with “N/A” to demonstrate that the question was considered but not applicable to this specific incident.
- Guess or estimate details about the crash; if certain information is unknown, it is better to note it as such rather than provide potentially incorrect data.
- Forget to include the involvement of commercial motor vehicles if applicable, as this requires additional information and documentation for compliance with state and federal regulations.
- Omit details about the crash environment, such as weather, lighting, and road conditions, as these factors can significantly impact the interpretation and understanding of how the incident occurred.
- Overlook the importance of documenting any witnesses or additional individuals involved but not injured, as their accounts may provide valuable insights into the crash.
- Use personal opinions or speculative language when describing the crash events; stick to factual and observable details only.
- Delay submitting the report beyond any stipulated deadlines to ensure timely processing and compliance with Virginia state law requirements.
Misconceptions
Misunderstanding the contents and requirements of the Virginia Police Crash Report form can lead to inaccuracies in reporting, potentially affecting the outcomes for those involved in traffic incidents. Correcting these misconceptions is crucial for accurate, complete crash documentation.
- Misconception 1: "The form is only for use in vehicle collisions."
Although vehicle collisions are a primary focus, the form also encompasses incidents involving pedestrians, cyclists, and property damage, making it a comprehensive tool for documenting a range of traffic-related incidents.
- Misconception 2: "All sections must be completed for every crash."
While thoroughness is important, not all sections apply to every incident. For example, the Commercial Motor Vehicle section is only required if the vehicle meets specific criteria such as weight or passenger capacity.
- Misconception 3: "Personal information reported is made public."
Personal details collected are used for official purposes and statistical analysis. Certain information may be redacted when reports are made available to the public to protect privacy.
- Misconception 4: "The report form is the same across all states."
Each state has its own form and requirements. The Virginia Police Crash Report form is specific to the Commonwealth of Virginia, tailored to meet state laws and data collection needs.
- Misconception 5: "Police officers decide who is at fault based on this form."
This form documents details of the crash without assigning legal fault. Fault determinations are typically made by insurance companies or through legal proceedings, not directly by the police.
- Misconception 6: "The form is not necessary if insurance is not involved."
Even if the parties involved choose not to involve insurance, completing the form is crucial for legal documentation and statistical purposes, helping to improve road safety measures.
- Misconception 7: "Only police can fill out the form."
While police officers complete this form at the scene of a crash, individuals can request a copy for their records or to provide additional information to insurance companies or legal representatives.
- Misconception 8: "You don't need to report minor crashes."
Virginia law requires crashes involving injury, death, or significant property damage to be reported. Thus, even seemingly minor crashes may need to be documented if they meet certain criteria.
Understanding these nuances ensures that the Virginia Police Crash Report form is completed accurately and effectively, providing a reliable record for involved parties, insurers, and state agencies.
Key takeaways
When filling out and utilizing the Virginia Police Crash Report form, it is crucial to pay attention to specific sections that require detailed and accurate information. Here are ten key takeaways to consider:
- Accurate details are essential: Ensure that incident details such as GPS coordinates, time, date, and location of the crash are recorded precisely to facilitate investigation and reporting accuracy.
- Vehicle information is critical: Document complete vehicle data including the year, make, model, license plate number, and Vehicle Identification Number (VIN) for all vehicles involved.
- Driver and passenger information: For every involved party, include driver’s names, addresses, license information, and any passengers’ details, especially if injuries were sustained.
- Injury and safety equipment: Record all injuries, the use, or the absence of safety equipment like seat belts or airbags, and whether they were activated or if ejections occurred.
For crashes involving commercial vehicles, it's imperative to note specific details such as the vehicle’s configuration, cargo type, carrier identification, and if hazardous materials were present. - Diagram and narrative: Provide a clear diagram of the crash scene and a thorough narrative description, including the sequence of events and the initial impact area to assist in understanding how the crash occurred.
- Weather, roadway, and lighting conditions: Document the environmental and roadway conditions at the time of the crash to identify possible contributing factors.
- Traffic controls and signage: Identify and record any traffic control devices or signs in place at the crash location, including their operational status.
- Cause and contributing factors: Detail the apparent cause of the crash and any contributing conditions or actions, such as speeding, vehicle defects, or driver impairment.
- Reporting requirements: Understand when the form must be submitted, especially if the crash involves fatalities, injuries, commercial vehicles, or requires tow-away, as different scenarios may have specific reporting obligations.
Ensuring the Virginia Police Crash as summary of the entire incident, facilitating accurate processing and reporting. Report form is filled out comprehensively and accurately not only aids in the immediate aftermath of a crash but also serves as a valuable document for legal, insurance, and statistical purposes. It provides a complete
Other PDF Forms
Virginia Court Forms - Advises on the importance of legal representation in understanding and navigating the effects of legal documents and orders in divorce.
Virginia Sales Tax Exemption - Streamlines the process for Virginia's public sector to obtain goods and services crucial for their operations, tax-free.
Wv Social Studies Fair - A project on health disparities in West Virginia, investigating causes, major health concerns, and efforts to improve outcomes.